


An expert in shoulder surgery clears up shoulder ailments
I receive patients at the Aava and Terveystalo medical centres in Helsinki and Espoo.
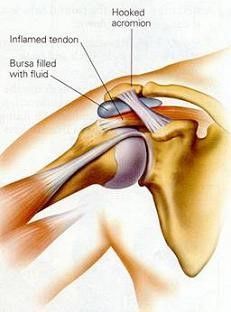
Impingement shoulder symptoms
Symptoms:
The shoulder hurts even with a small amount of repetitive strain, and upper body exercises and movements above shoulder level become problematic in the gym. Putting a shirt into your pants behind your back hurts. The friction can cause inflammation of the tendon and bursa, which causes stiffness and pain when lying down. The pain is often felt in the upper arm, even though the cause of the pain is in the shoulder joint.
TREATMENT:
A symptom that is caused by functional muscular imbalance and stiffness can be treated successfully through physiotherapeutic methods – with stretching and motion exercises. Motion exercises and stretches must be done strictly according to the instructions, in order to achieve the best result. In situations of acute pain, anti-inflammatory drugs and occasional cortisone injections often bring relief. All movements that chafe at the shoulder level should be avoided, and the paths of motion of the shoulder should be limited to below shoulder level until the inflammation caused by the chafing has calmed down. If there is a structural impingement behind the ailment, the syndrome will arise again intermittently, and in this case arthroscopy on the shoulder joint has to be considered. In arthroscopy on the shoulder joint, more room is made for the tendon through three 5 mm-sized holes by removing bone from the front part of the acromion, as well as chafing soft tissue (acromioplasty). Recovery from this procedure is normally quick because usage of the arm is permitted right after it, depending on pain, and a sling is not needed at all. It is possible to return to office work as soon as the pain allows, generally about 1-2 weeks after the procedure. Returning to leisure pursuits can happen when paths of motion have been restored, in about 3-4 weeks. Stitches do not have to be removed because the small arthroscopy holes can be closed with dissolvable stitches. There will be a check-up visit at the surgery within four weeks of the operation.
Tendon inflammations (tendinitis)
Tendon inflammations of the shoulder typically arise through overexertion and incorrect movements. Raking in the autumn and cleaning windows in the spring bring patients to the surgery due to sore shoulders. Swimmers and practitioners of over-the-shoulder sports irritate the tendons of the rotator cuff with incorrect techniques, causing inflammations. A tendon inflammation of the shoulder can also arise through an injury when the tendon and the bursa on top of it are squeezed against the acromion when falling or in connection with a wrenching incident.
Symptoms:
The inflamed tendon and bursa swell, causing pain when lifting the upper arm to the side. The pain occurs when the swollen and inflamed tendon presses against the shoulder joint above it during lateral lifting. This is the same reason why the shoulder hurts at night when lying down. The pain is often localized to the upper arm on the side and it becomes impossible to raise the arm up.
TREATMENT:
Treatment naturally includes calming down the inflamed and irritated tendon with rest and a course of anti-inflammatory drugs. Cold compresses a few times a day alleviate the pain. All movements that chafe the tendon at shoulder level should be avoided as long as the pain lasts. Shoulder stretches are not appropriate in the treatment of acute inflammation. If medication and rest do not bring relief within a week, a cortisone injection can be administered to the bursa on top of the inflamed tendon. This eases the pain in most cases within a few days. Individual cortisone injections do not have a harmful effect on the bones or the tendons of the rotator cuff, as is often erroneously supposed. Returning to leisure pursuits or over-the-shoulder sports should happen step by step, paying attention to the pain. Calcific deposits may also accumulate in the tendon through the inflammation, in which case the syndrome is often quite intense. Restrictions to movement are significant and sleep at night is disrupted. The calcific deposits show up clearly in X-ray imaging. In these cases, the worst pain symptom can be curbed through a calcific deposit removal done with the aid of ultrasound guidance. Cortisone is often used in conjunction with this to calm down the inflammation. The body can also remove the calcific deposits itself, but this takes time. If the calcific build-up is not removed despite all these measures, the symptoms can be alleviated through an arthroscopic procedure in which the calcific deposits are removed and, at the same time, the passage of the tendon is also widened.
Pain symptom of the biceps tendon
The biceps muscle is firmly attached to the coracoid in the top part of the upper arm. The other so-called long tendon of the biceps goes around the front of the shoulder in a narrow bony groove, attaching to the top edge of the elbow cavity. In its bottom part, the biceps muscle is attached to the radius in the top part of the forearm.
Biceps tendon ailments, such as ruptures or fraying, can also manifest themselves as different kinds of shoulder pain states. A rupture usually does not require surgical treatment, only time. Fraying, on the other hand, may require treatment: either cutting or reattachment. An expert orthopaedist can advise you on the right option.
Biceps tendon inflammation:
Symptoms relating to the long tendon of the biceps are particularly common with people who do throwing sports as well as swimmers. The tendon chafes in its bony groove through repeated movements and may become inflamed. Symptoms include pains that are localised in the front part of the shoulder. Lifting motions done from the front with an extended upper limb are painful. The biceps tendon is often also tender when pressed in the top part of the upper arm in its bony groove. Treatment naturally includes calming down the inflamed and irritated tendon with rest and a course of anti-inflammatory drugs. Cold compresses a few times a day in the shoulder area alleviate the pain. In the case of a prolonged inflammation, cortisone injections are also used to calm down the inflammation.
Luxation of the biceps tendon:
In association with a wrenching injury of the shoulder or a fall, the structures that keep the biceps tendon in its bony groove may be damaged. Due to this, the tendon tries to slip out of the groove when turning the upper limb in an external rotation. Symptoms are pain or a clear intermittent popping sound in the front part of the shoulder, particularly in association with external rotations of the upper arm. The syndrome also often includes tearing of the subscapularis tendon. Tennis serves and throwing become impossible because of the pain. Treatment in the initial stage is alleviating the inflammatory reaction and pain after the injury, and restoring paths of motion through physiotherapeutic methods. After this, it will be assessed whether detrimental symptoms will remain. In surgical treatment of a tendon that is trying to move out of position, the tendon can be reattached to the top part of the upper arm. If the tendon is in a bad condition due to fraying, it can simply be cut. Together with the cutting, the shape of the biceps changes a little, but the action does not cause functional detriment as such – the biceps muscle is still firmly attached to the coracoid. In the case of young, active people, the primary aim is to reattach the tendon.
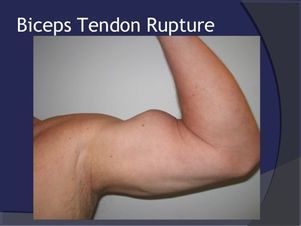
Biceps tendon rupture:
The long tendon of the top part of the biceps is, while moving in its bony groove, subject to chafing, inflammation and the degeneration of the tendon. Through this, the tendon often gets weaker, frays and splits lengthways over time. A rupture of the tendon in conjunction with an exertion is very common with elderly people. Due to the rupture, the shape of the biceps turns into a so-called Popeye muscle. The pain stage normally lasts for a few weeks, after which the shoulder usually recovers to normal in stages and no functional detriment remains. Motions that encumber the biceps should be avoided for about a month so that no annoying muscle cramp presents itself. A tear in the upper part of the biceps tendon is hardly ever treated through surgery. The lower part of the biceps detaching from the radius typically happens when carrying a heavy burden with an outstretched limb. The most common situations are, for example, tears that occur through a slight stumble when carrying a washing machine in a staircase. The pain is localised in the area of the crook of the elbow and the biceps muscle rises. These tendon detachments of the bottom part of the biceps are fixed through surgery. Personally, I have used so-called double attachment in these operations, which makes moving the upper limb possible right after the operation and returning to work unencumbered is possible as early as one week after the operation. Actual muscle exercises for the biceps should only be begun three months after the operation. If operated on using the older techniques, the arm is kept in a sling for four weeks, on account of which recovery is considerably slower.
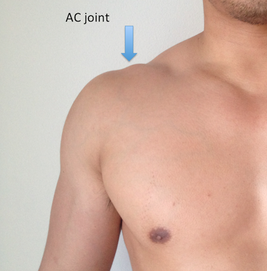
Shoulder-clavicle joint pain symptom (AC joint)
Causes and symptoms:
The clavicle is joined to the acromion of the shoulder blade above the shoulder. This joint typically manifests symptoms when reaching with the arm to the other side of the body, lifting heavy weights from below and in the bench-press movement. The pain is localised on top of the shoulder in the tender and often slightly swollen spot where the joint is. The ailment is particularly common with those who practise weight-lifting actively. The pain may be caused by wear in the joint that arose through an old shoulder injury, an inflammation, or prolonged pain symptoms after an injury due to cartilage damage. The cause of the ailment can often be determined just through a careful examination. With prolonged and repeated pain symptoms, the matter is clarified through imaging methods, either with X-rays or MRI scans.
Treatment:
The treatment of an AC joint that has become painful through strain involves calming down the inflammation with cold compresses, anti-inflammatory drugs and avoiding strain. A cortisone injection is often a useful aid with this ailment as well. However, the relief will often be only a temporary one if there is a structural cause in the joint that makes it susceptible to pain. An arthroscopic surgery, however, may help get rid of a long-lasting and bothersome ailment. Through three 5 mm-sized holes, the joint is opened up from below and the scarring is removed from the joint space, along with a few millimetres from the end of the clavicle, through which the previously symptomatic joint space becomes free in movement. After the procedure, use of the upper limb is permitted at once, depending on pain, nevertheless avoiding heavy encumbrance for about four weeks.
Frozen shoulder (capsulitis)
A frozen shoulder involves an inflammation of the joint capsule that surrounds the shoulder joint. Through this, the capsule thickens and scars, leading to stiffening of the shoulder joint. The average duration of the disorder is from one to two years and it causes considerable hindrance to coping with everyday life. However, the good thing about this is that the functionality of the shoulder usually returns to its previous state after recovery. The root cause for the inflammation is often not known; it is most prevalent amongst diabetics and cases where the thyroid gland is underactive (hypothyroidism). A wrenching injury to the shoulder or a shoulder operation may also make you susceptible to capsulitis.
Symptoms:
The disorder can roughly be divided into three stages. In the first inflammation stage, the shoulder is very tender in all movements, also below shoulder level. Unlike in the case of tendon inflammation, rotational movements of the shoulder happening near the body at a lower level also cause pain. Sudden corrective movements, for example when staggering on a coach or tram, have a strong effect. Aching at night is typical. This inflammation stage lasts 3-6 months, during which a progressive restrictedness of movement appears. What is typical is stiffness specifically associated with rotational movements; rotating the arm to behind the back and outwards is restricted first, followed by abduction movements. When moving the arm to the side, the whole shoulder starts turning with it. As the inflammation calms down in the second stage, the pains gradually subside but the restrictedness of movement and stiffness do not. Most often, it is not possible to raise the arm above shoulder level at all, and in everyday life visits to the toilet, for example, are challenging. The shoulder still hurts under strain and when attempting extreme movements. This stage also lasts 3-6 months depending on the case. In the third stage, the paths of motion of the shoulder finally begin to return slowly but surely and there is light at the end of the tunnel. All in all, it can take up to two years from the beginning of the symptoms for the paths of motion to return to normal. A frozen shoulder can be diagnosed by asking thorough questions about the symptoms and through the examination conducted at the surgery. Imaging examinations are very rarely needed.
Treatment:
Unfortunately, the duration of the disorder cannot be shortened by medication or other means. With treatments, the primary aim is to alleviate the symptoms and prevent a deterioration in the restrictedness of movement. In the inflammation stage, active stretching exercises should be avoided, even just because of the pain. Anti-inflammatory drugs are used according to need; long courses are of no benefit. If the aching at night is difficult, a cortisone injection can be administered. It should preferably be administered under ultrasound guidance because the drug is introduced inside the joint, unlike in the case of tendon inflammations. For some patients, this helps curb the worst pain.
Is your shoulder bothering you? Get in touch and book an appointment with shoulder surgeon Ilkka Moilanen, who operates in Espoo and Helsinki!
BOOK AN APPOINTMENT CONVENIENTLY ONLINE!
OPEN
SURGERIES OF SHOULDER SURGEON ILKKA MOILANEN:
Terveystalo Leppävaara
Terveystalo Ruoholahti
Aava KamppiAava Ortho-Doctors, tel. 010 380 5200
Animation of a rotator cuff tear