


Shoulder injuries - specialist in Helsinki and Espoo
Is your shoulder bothering you? Pain or other discomfort can be caused by many different reasons. It can be, for example, trauma-related or caused by strain. I specialize in shoulder surgery, so you can get solutions to your problems from me. When your shoulder is bothering you, you can trust the expertise of a shoulder surgeon.
On this page you will find information about various shoulder problems and their treatments.
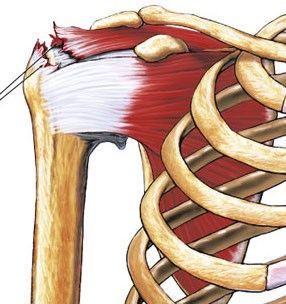
Rotator cuff tear (tendon tear)
The shoulder joint is surrounded by a rotator cuff made up of four tendons. With this, we can raise and rotate the arm in different directions. Rotator cuff injuries most often come about when falling onto an extended limb, when the arm is wrenched hard and sometimes through extreme exertion.
SYMPTOMS:
Through falling or wrenching, the shoulder becomes painful, and in the initial stage the pain may cause restricted movement. The pain often radiates to the top part of the arm and raising the arm sideways does not work because of the pain. Cold compresses, rest and anti-inflammatory drugs are home treatments in the initial stage. The pain and inflammatory reaction after a sprain injury usually subside within two weeks, but if the shoulder pain is prolonged, you should see an orthopaedist for an assessment. At the surgery, the shoulder is examined through numerous tests and it is decided whether an X-ray or MRI scan is needed as a further examination.
TREATMENT:
A complete tear of the rotator cuff that has resulted from an accident is treated, as a rule, through surgery on those of working age. With extensive tears, the arm is left restricted in terms of movement as well as strengthless, and a three-week monitoring period can be considered the limit: if the limb does not independently rise above the level of the shoulder within this period, it should be examined. If left untreated, permanent atrophy and disability develops in the musculature of the shoulder. The torn edge of the tendon is left in the constricted intermediate space of the shoulder to chafe and snag against the acromion. The line of treatment for partial tears of the tendon is affected by many operational and structural factors. The situation may often just be monitored while the paths of motion are worked on through physiotherapeutic means. These days, surgical treatment of shoulder tendon damage is almost always done arthroscopically through 5 mm-sized holes. The procedure requires a great deal of experience and an experienced surgeon to achieve a good end result. In conjunction with the corrective work on tendons, the lower part of the acromion can be polished down at the same time, thus making room for the pathway of the tendon. Stitches do not have to be removed because the small arthroscopy holes can be closed with dissolvable stitches.
REHABILITATION:
Although the tendon repair itself is quick, time must be set aside for rehabilitation. After tendon repair, the upper limb is kept in a sling for a total of 6 weeks. During this time, the tendon is fixed to its original position through scarring. Physiotherapy begins 4 weeks after surgery, and a check-up visit is also held at the doctor who performed the surgery. The sling can be removed when showering and a couple of times a day to allow the elbow joint to be stretched. However, all load-bearing movements should still be avoided. When 6 weeks have passed since the surgery, the sling can be removed and independent shoulder exercises (so-called active movement exercises) can be gradually started under the guidance of a physiotherapist. Rehabilitation from tendon repair often takes 6-12 months in total. The period of disability largely depends on the profession and which hand has been damaged. Some people return to office work with a sling 2 weeks after surgery, but they do not return to physically demanding jobs until about 3 months after surgery.
Dislocated shoulder joint (luxation)
Dislocation of the shoulder joint most commonly occurs when falling on an outstretched upper limb. The shape of the shoulder changes visibly as the humerus falls forward and down. Nearby nerve structures can be stretched with the injury, and therefore the shoulder joint should be put back in place quickly. Dislocation of the shoulder joint causes different injuries in different age groups. In young people, the cartilage ring that lines the socket often comes off, and this can lead to looseness of the joint and repeated dislocations. Without surgery, the risk of re-dislocation is approximately 70% in young people who are actively involved in sports. Fractures on the edge of the socket and cartilage damage are also often found. In these cases, the treatment line is decided on a case-by-case basis between surgery and rehabilitation.

TREATMENT:
Immediate treatment is to immobilize the shoulder by hanging or manipulating it. X-rays are often necessary to rule out fractures. After this, the upper limb is kept in a sling along the body for 1-2 weeks. After about three weeks, exercise can be started, but external rotation should be avoided for 6 weeks to allow the damaged joint capsule to recover. At a follow-up visit after about 6 weeks, the range of motion and possible looseness can be tested. Magnetic resonance imaging is invaluable in identifying structural damage. If the shoulder joint remains loose and symptomatic, endoscopic surgery is considered, in which the detached cartilage ring is fixed in place using wire anchors.
To ensure fixation, the upper limb is kept in a sling for 3 weeks. After this, physiotherapy-guided rehabilitation begins to restore range of motion. Suture removal is not necessary, as small endoscopic openings can be closed with dissolvable sutures. A follow-up visit to the office is held 4 weeks after surgery. The sick leave period depends on the profession and the inconvenience caused by the sling. It is possible to return to office work three weeks after surgery. The overall recovery from this surgery takes about 3 months, after which the patient can gradually return to sports. In older patients, dislocation almost always leads to a rotator cuff tear, which often goes unnoticed in the early stages. Therefore, a follow-up visit to the office after the injury is necessary to ensure rehabilitation and, if necessary, to schedule further examinations.
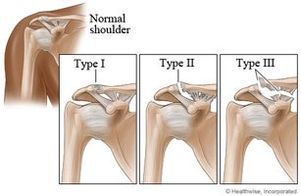
Dislocated collarbone (AC dislocation)
Injuries to the head of the clavicle typically result from falling on one’s side with the elbow stretched out. The injury is common in ice hockey in side tackles, in combat sports and, for example, when falling while cycling. A symptom of mild-degree injuries is that the joint capsule is swollen and sore in movement from a week to two weeks. The pain in these injuries is localised on top of the shoulder where this joint is. If the energy of the injury is great, the head of the clavicle may rise completely out of the joint, in which case the ligaments that support the joint also tear. In these so-called fourth-degree tears, the head of the clavicle becomes free to move backwards and forwards as well in connection with the movements of the arm, often causing significant pain symptoms.

TREATMENT:
With mild-degree injuries, a sling will be used during the period of pain, as well as cold compresses and anti-inflammatory drugs. The AC joint is particularly encumbered in bench-pressing, when lifting heavy weights from the floor and in reaching exercises that stretch across the body, such as the movements done with a diagonal pulley. These should be avoided, depending on the degree of the injury, for one to four weeks. In the case of fourth-degree injuries, operative treatment becomes necessary. With new injuries, the head of the clavicle is fixed in place in arthroscopic surgery, and a sling is worn for four weeks to ensure the attachment. In delayed situations, the torn ligaments are replaced with a tendon transplant in conjunction with the operation. Rehabilitation for sport takes, depending on the sport in question, about four months.
Biceps tendon injuries
The biceps muscle attaches firmly to the coracoid process at the top of the upper arm. Another, the so-called long biceps tendon, loops in a narrow bony groove at the front of the shoulder inside the joint, attaching to the upper edge of the glenoid fossa. At its lower end, the biceps muscle attaches to the upper part of the forearm, to the radius bone.
BICEPS TENDON INFLAMMATION:
Symptoms of the long tendon of the biceps are common, especially in athletes who practice throwing sports and swimmers. The tendon rubs in its bony groove with repetitive movements and may become inflamed. Symptoms include pain localized to the front of the shoulder. Lifting movements performed from the front with the upper limb extended are painful. The biceps tendon is often also tender when pressed in its bony groove in the upper arm. Treatment is naturally to soothe the inflamed and irritated tendon with rest and a course of anti-inflammatory medication. Cold baths a few times a day in the shoulder area relieve pain. In prolonged inflammation, cortisone injections are also used to calm the inflammation.
Biceps tendon problems, such as rupture or fraying, can also manifest as various shoulder pain conditions. A rupture usually does not require surgery, just time. A fraying, on the other hand, may require treatment: either rupture or reattachment. An expert orthopedist can advise on the right option.
LUXATION OF THE BICEPS TENDON:
In association with a wrenching injury of the shoulder or a fall, the structures that keep the biceps tendon in its bony groove may be damaged. Through this, the tendon tries to slip out of the groove when turning the upper limb in an external rotation. Symptoms are pain or a clear intermittent popping sound in the front part of the shoulder, particularly in association with external rotations of the upper arm. The syndrome also often includes tearing of the subscapularis tendon. Tennis serves and throwing become impossible because of the pain. Treatment in the initial stage is alleviating the inflammatory reaction and pain after the injury, and restoring paths of motion through physiotherapeutic methods. After this it is assessed whether detrimental symptoms will remain. In surgical treatment of a tendon that is trying to move out of position, the tendon can be reattached to the top part of the upper arm. If the tendon is in a bad condition due to fraying, it can simply be cut. Together with the cutting, the shape of the biceps changes a little, but the action does not cause functional detriment as such – the biceps muscle is still firmly attached to the coracoid. In the case of young, active people, the primary aim is to reattach the tendon.
BICEPS TENDON RUPTURE:
The long tendon of the top part of the biceps is, while moving in its bony groove, subject to chafing, inflammation and the degeneration of the tendon. Through this, the tendon often gets weaker, frays and splits lengthways over time. A rupture of the tendon in conjunction with an exertion is very common with elderly people. Due to the rupture, the shape of the biceps turns into a so-called Popeye muscle. The pain stage normally lasts for a few weeks, after which the shoulder usually recovers to normal in stages and no functional detriment remains. Motions that encumber the biceps should be avoided for about a month so that no annoying muscle cramp presents itself. A tear in the upper part of the biceps tendon is hardly ever treated through surgery. The lower part of the biceps detaching from the radius typically happens when carrying a heavy burden with an outstretched limb. The most common situations are, for example, tears that occur through a slight stumble when carrying a washing machine in a staircase. The pain is localised in the area of the crook of the elbow, and the biceps muscle rises. These tendon detachments of the bottom part of the biceps are fixed through surgery. Personally, I have used so-called double attachment in these operations, which makes moving the upper limb possible right after the operation and returning to work unencumbered is possible as early as one week after the operation. Actual muscle exercises for the biceps should only be begun three months after the operation. If operated on using the older techniques, the arm is kept in a sling for four weeks, on account of which recovery is considerably slower.
Shoulder fractures
Fractures of the upper part of the arm result from falling. The pain is usually so intense that it drives patients to scans and treatment in good time. Bruising often appears on the skin and moving the arm is not possible because of the pain.
TREATMENT:
The line of treatment is defined on the basis of X-ray imaging. Fractures that are in a good position are taken care of with a sling for about three weeks, after which guided motion exercises are begun in physiotherapy. Restoration of the range of motions takes many months and, as a result of the fracture, even permanent restrictedness of movement may remain in the case of extreme motions. The tendons attached to the edge of the head of the humerus may also detach a piece of bone when falling. In these cases, the tendon may pull the piece of bone with it into the intermediate cavity of the shoulder, causing a mechanical obstacle to movements. An ordinary X-ray is a sufficient examination. A fracture of the tendon attachment area always requires surgical treatment. Fractures of the joint cavity usually arise in conjunction with dislocation of the shoulder and the line of treatment is decided on the basis of the size and displacement of the fracture piece. Some fractures that require surgery can be done through an arthroscopic technique.
Clavicle fractures
Clavicle fractures occur when falling on your side with your shoulder first. A bruise forms in the fracture area, and the pain drives you to see a doctor. The course of treatment is decided based on an X-ray. Clavicle fractures usually heal well, which has led to them often being treated without surgery with a sling for 4 weeks. If the fracture is allowed to heal in an incorrect position, the result is a permanent bone ridge under the skin, which often causes problems, for example when carrying a backpack when the shoulder strap rubs against the skin. Early surgical treatment can avoid these problems by placing the ends of the bone in their natural position.

Problems with your shoulder? Get in touch and book an appointment with shoulder surgeon Ilkka Moilanen, who operates in Espoo and Helsinki!
BOOK AN APPOINTMENT CONVENIENTLY ONLINE!
SURGERIES OF SHOULDER SURGEON ILKKA MOILANEN:
Aava Kamppi
Aava Orto-Lääkärit, tel. 010 380 5200
Terveystalo Ruoholahti
Terveystalo Leppävaara
Animation of a rotator cuff tear